
Dr. Pranai Tandon, Assistant Professor of Pulmonary and Critical Care Medicine and clinical expert for the Clinical Data Science team, has been awarded the Dean’s Team Science Award for the “Respiratory Insights: Improving the Management of Respiratory Failure with Analytics and AI” submission.
This Team Science award is meant to recognize an outstanding interdisciplinary or transdisciplinary research team for its innovative and impactful science that has advanced or likely will advance the detection, diagnosis, prevention or treatment of disease. This research effort should: 1) represent a partnership between basic and clinical scientists from different (unrelated) Departments and/or Institutes (at least 2); 2) reflect a novel undertaking that would not have been accomplished by any single member of the team working in isolation; and 3) involve tackling a unique challenge in medicine. Teams that have intentionally included outreach to the community or to specific patient populations related to the research undertaking or have included community members as part of the team, will be additionally noted. We strongly encourage applications from research teams that reflect postdoctoral trainee contributions and additionally integrate community stakeholder perspectives and partnership. Submissions must be responsive to these specified requirements.
Below is a brief summary of the submission:
Respiratory Insights: Improving the Management of Respiratory Failure with Analytics and AI
Pranai Tandon MD1,2, Kim-Anh-Nhi Nguyen MS2, Ganesh Raut MS2, Shamsuddoha Ranginwala RRT-NPS3, Prathamesh Parchure MS2, Gary Oldenburg MS, RRT-NPS3, Neha N. Goel MD1, Prem Timsina ScD2, Matthew A. Levin MD2,4,5, Robert Freeman DNP2, Charles A. Powell MD, MBA1.
1 Division of Pulmonary, Critical Care, and Sleep Medicine 2 Mount Sinai Clinical Data Science Team 3 Respiratory Care Services 4 Department of Anesthesiology, Perioperative, and Pain Medicine, 5 – Department of Artificial Intelligence and Human Health
Clinical Problem: For critically ill patients with acute respiratory failure requiring invasive mechanical ventilation, Lung Protective Ventilation (LPV) with tidal volumes <=8cc/kg predicted body weight and controlled ventilator plateau and driving pressures remains one of the few interventions proven to reduce mortality. Despite broad awareness of this essential practice, fewer than 20% of patients consistently receive standard of care LPV. To address this gap, our interdisciplinary team of Pulmonary and Critical Care Physicians, Respiratory Therapists, and Clinical Data Scientists created Respiratory Insights.
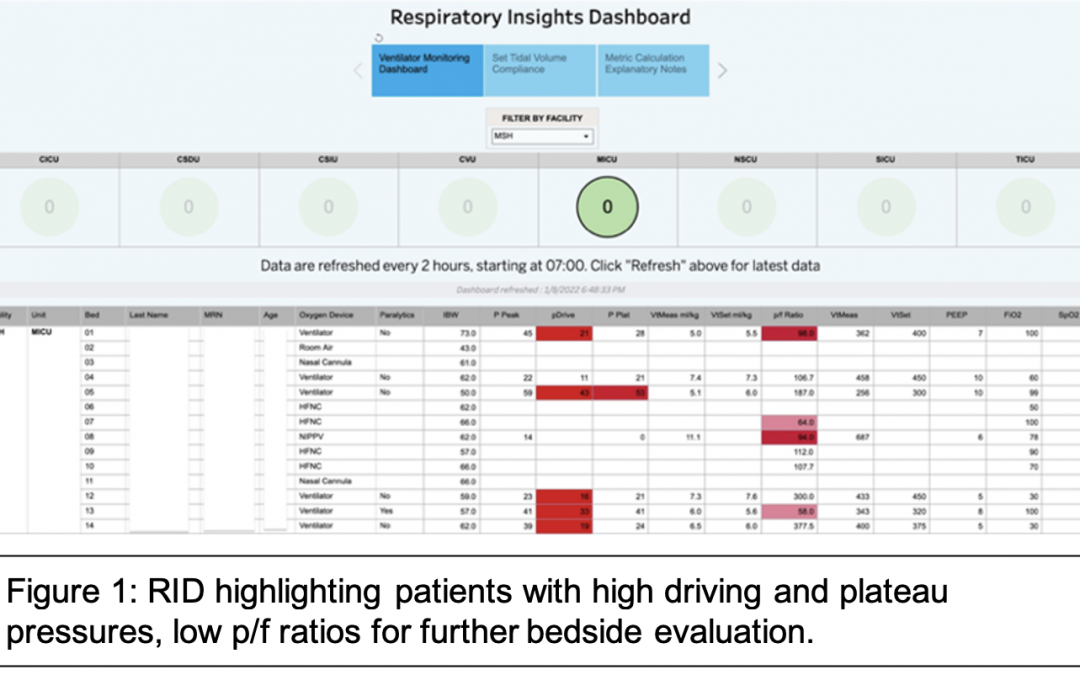
Innovation and Intervention: The Respiratory Insights Dashboard (RID, Figure 1) is a real-time patient monitoring and analytics solution which uses streaming data to continuously monitor all ICU patients on invasive mechanical ventilation throughout the Mount Sinai Health System. The platform synthesizes key information in a visual dashboard, flags patients with unsafe ventilator settings, and sends e-mail alerts to bedside ICU clinicians and respiratory therapists at the beginning of each shift summarizing flagged patients with out-of-bound parameters for intervention (Figure 1). Bedside respiratory therapists can then review flagged patients and make appropriate adjustments in conjunction with critical care clinicians. The RID, built on the MSHS Clinical Data Science Platform with data visualization in Tableau, can integrate with any ventilator manufacturer and any EHR, and is available via website, mobile app, and summary emails for convenient review. To facilitate continuous improvement, the RID automatically calculates and trends Key Performance Indicators (KPIs) for lung protective ventilation – these KPIs are reviewed regularly by respiratory care management to ensure program success. Continuous automated monitoring with active alerts is unique in ventilator management.
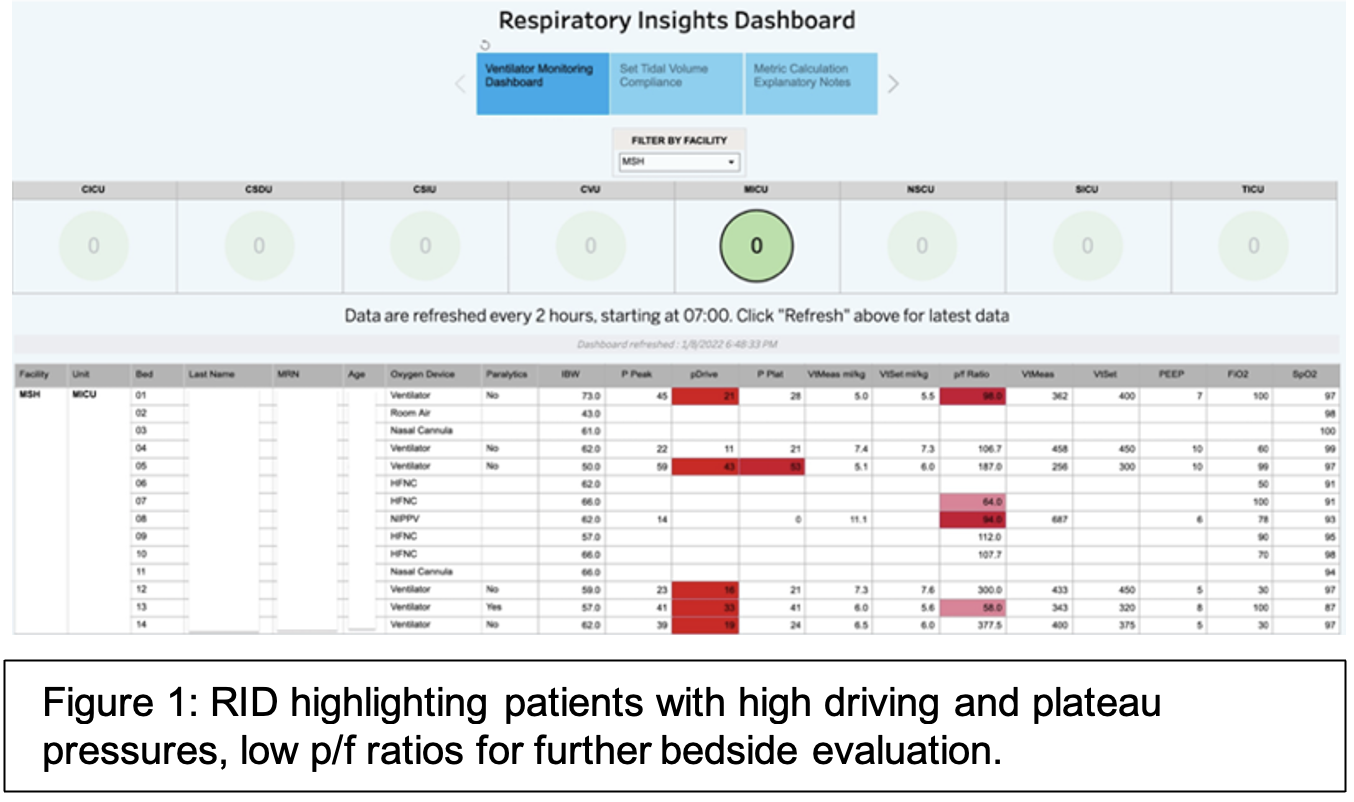
Clinical Impact: First deployed at the Mount Sinai Hospital in 2020, the RID resulted in an 11.5% improvement in LPV adherence and a 44% decrease in the time to correct unsafe ventilator settings. In 2021 the RID was scaled to include Mount Sinai Morningside, Mount Sinai West, Mount Sinai Queens, Mount Sinai Beth Israel (now closed), and Mount Sinai Brooklyn. Across these 5 additional centers, RID deployment resulted in sustained improvement in LPV adherence from 76% to 85% (p<0.001) and decreased time to ventilator adjustments from a median of 18 to 9 hours (p<0.001). Median Daily Driving Pressure fell from 16cmH2O to 12cmH2O (p<0.001). Interrupted time-series regression (Figure 2) demonstrated a significant and sustained improvement in LPV metrics. Analysis on further outcomes such as mortality, ventilator days, and length of stay are underway. This work has been academically impactful with two presentations at the American Thoracic Society International Conference, and a manuscript in CHEST: Critical Care1–3.
Team Science Model: Respiratory Insights was initiated by clinical investigators and bedside clinicians who identified persistent gaps in the real-world delivery of lung protective ventilation despite strong evidence. The project was intentionally designed as a transdisciplinary team science effort integrating clinical investigators, respiratory therapists, and clinical data scientists. Respiratory therapists are key stakeholders who operationalize the platform’s outputs, translating analytic alerts into real-time bedside ventilator adjustments in partnership with ICU physicians. The data platform, analytics, and visualizations were developed through an iterative co-design process, with continuous feedback between clinicians and data scientists to ensure clinical relevance, usability, and scalability. This collaboration has also served as a training environment for translational investigators, mentoring fellows who are now early-career faculty supported by or pursuing mentored career development awards (Goel, Tandon). This same framework will supports ongoing initiatives developing and translating clinical AI tools to the bedside to optimize the management of respiratory failure.
Scalability and Longevity: The RID has been scaled to cover all ICUs in 5 hospital centers and has demonstrated sustained engagement since 2021 with more than 150 daily clinical users across MSHS.
Upcoming Initiatives: Based on our success in optimizing lung protective ventilation, our group is extending our platform and collaborating on several new patient safety and health system efficiency initiatives:
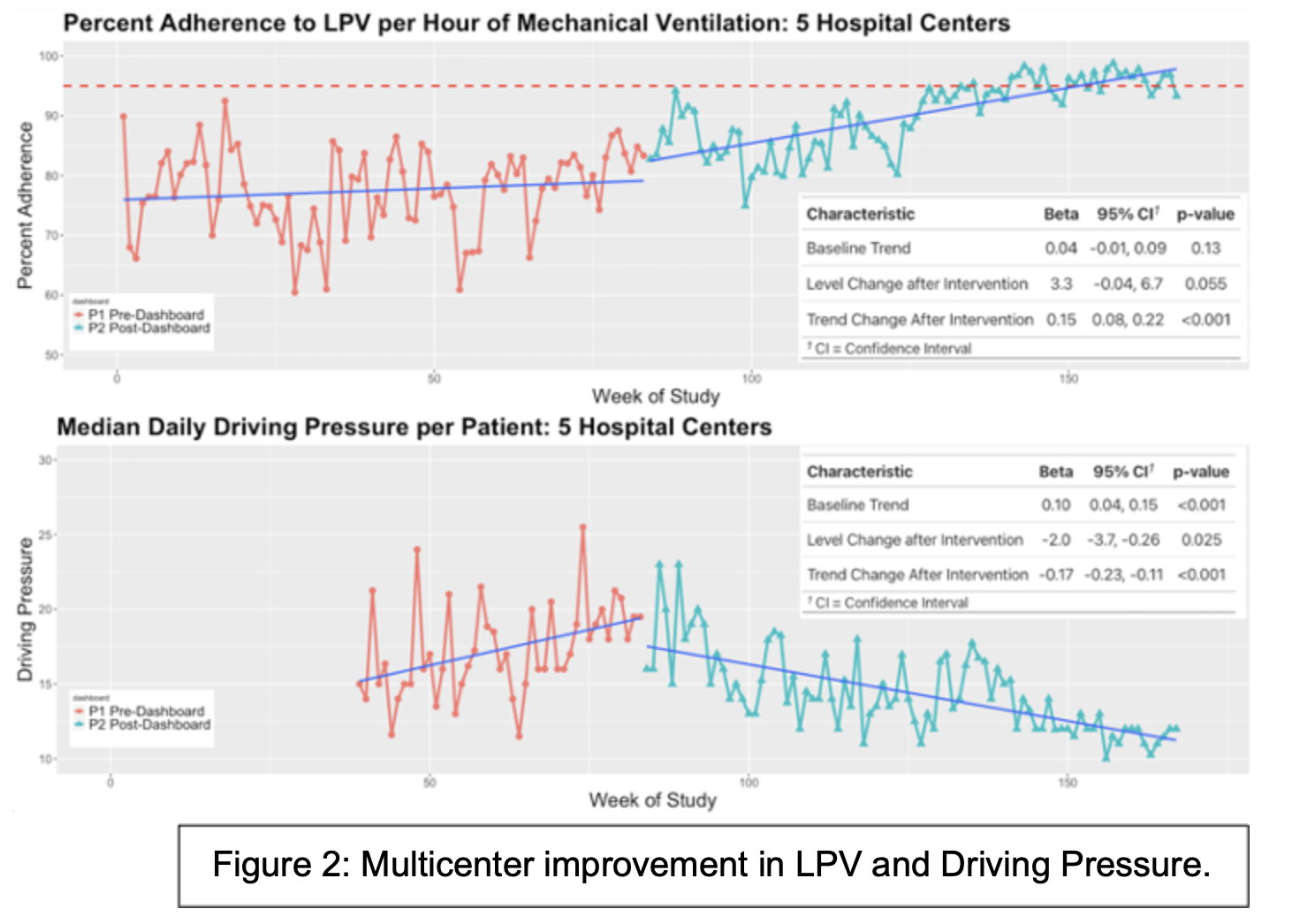
• Monitoring Non-Invasive Ventilation – A dashboard and alert system monitoring patients with acute respiratory failure on high-flow nasal cannula for indications for intubation (Figure 3). Patients at elevated risk of respiratory decompensation are flagged for further evaluation and escalation by the treatment team. This initiative is in a pilot at MSH.
• Optimizing Ventilator Liberation – An ML model identifying patients for early and intensive ventilator weaning to reduce ventilator-days and ICU length of stay. This predictive engine is under evaluation at MSH. This work is also academically impactful with presentations at the ATS International Conference, the SCCM Critical Care Congress, and a manuscript in Bioengineering4–7.
Conclusions: Respiratory Insights has resulted in sustained long-term improvements in the delivery of LPV across the health system to levels far above peer institutions and facilitated precision management of mechanical ventilation with driving pressure guided ventilator adjustment. Further work will span the entire gamut of respiratory failure, from optimizing non-invasive respiratory support, optimizing ventilator settings, and facilitating liberation from the ventilator. Critically ill patients with respiratory failure on invasive and non-invasive life support are among the most vulnerable under our care. This team collaboration exemplifies Mount Sinai as a learning health system, translating continuous data into actionable insights and improving patient care.
References
1. Tandon P, Nguyen K-A-N, Raut G, et al. Impact of a Real-Time Ventilator Management Dashboard With Alerts: Sustained Hospital-Wide Improvement in Lung Protective Ventilation. CHEST Crit Care 2025;3(4):100167.
2. Tandon P, Nguyen K -a.-N, Raut G, et al. Multicenter Deployment of a Real-time Ventilator Management Dashboard With Alerts: Sustained Improvement in Lung Protective Ventilation in 5 Hospital Centers [Internet]. In: C22. CLINICAL AND TRANSLATIONAL STUDIES IN MECHANICAL VENTILATION. American Thoracic Society; 2023 [cited 2026 Jan 22]. p. A4572–A4572.
3. Tandon P, Nguyen K -a.-N, Rajendran M, et al. Deployment, Adoption, and Clinical Impact of a Real-Time Ventilator Management Dashboard [Internet]. In: TP55. TP055 MECHANICAL VENTILATION, ICU MANAGEMENT, AND CV. American Thoracic Society; 2021 [cited 2026 Jan 22]. p. A2815–A2815.
4. Tandon P, Nguyen K-A-N, Edalati M, et al. Development and Validation of a Deep Learning Classifier Using Chest Radiographs to Predict Extubation Success in Patients Undergoing Invasive Mechanical Ventilation. Bioengineering 2024;11(6):626.
5. Nguyen K-A-N, Tandon P, Edalati M, Kia A. 360: A DEEP LEARNING MODEL USING CHEST X-RAYS TO PREDICT REINTUBATION RISK IN CRITICAL CARE. Crit Care Med 2024;52(1):S154.
6. Tandon P, Cheng F-Y, Cheetirala SN, Parchure P, Levin M, Kia A. Predicting Readiness to Liberate from Mechanical Ventilation Using Machine Learning: Development and Retrospective Validation [Internet]. In: TP54. TP054 MECHANICAL VENTILATION. American Thoracic Society; 2021 [cited 2021 Oct 28]. p. A2757–A2757.
7. Shpiner A, Chandra S, Zietlow E, et al. Evaluation of User Attitudes Affecting Adoption of a Machine Learning Decision Support Tool for Ventilator Weaning. Am J Respir Crit Care Med 2025;211(Abstracts):A5577–A5577.